"Orgasm in women with spinal cord injuries: a laboratory-based assessment." Sipski ML1, Alexander CJ, Rosen RC. Arch Phys Med Rehabil. 1995 Dec;76(12):1097-102.
Hello, welcome again to A Journal Article I Read! As always, I will do my best to give you a comprehensive understanding of this study as quickly as possible and without getting too bogged down in confusing language and details. Unless I specifically tell you I'm giving my opinion, then assume I am paraphrasing the study. Also, if you have any additional thoughts or corrections or anything else, please let me know. I would love to hear from you.
This one is a 1995 article investigating orgasm in women with spinal cord injury. This team has a few articles investigating this, but this is one of their earlier ones. I think they're doing some important work here that I imagine is quite hopeful and useful for women with these types of injuries.
I am particularly interested in this article for a couple reasons:
1. It investigates ability to orgasm among women with a variety of spinal cord injuries (SCI), so it has at least a little something to say about the mechanism and pathway for female orgasm in general.
2. It investigates orgasm in women with SCI in a different way than the Komisaruk article on the same topic that happens to get much more play in the media
3. It takes data on pelvic muscular activity at time of orgasm, but does not include that data in the results except to comment on whether the ability to have voluntary rectal contractions was related to rectal contractions (indicating pelvic muscular activity) at time of orgasm (they are not significantly related).
If you read my blog, you know I'm always going on about problems associated with lady-gasm studies not taking the time to discern between orgasm claims that include rhythmic pelvic muscular activity at time of orgasm and orgasm claims that do not include that muscular activity. Anyway, it's super interesting that this study took the time to gather data on pelvic muscular activity but didn't incorporate it into the results...and didn't say why.
MY QUICK INTRO THOUGHTS
In general, I think this is a well done and important study showing that women with SCI are more able to orgasm than previously thought and can achieve orgasm through genital self-stimulation. However, as is so often the case with female orgasm studies, it relies on women simply saying that they have orgasmed in order to deem a masturbation session as orgasmic or not. It does not discern whether all of those claimed orgasms are physically identifiable through rhythmic pelvic muscular activity at the time of orgasm or not. It only uses heart rate, respiration rate, and blood pressure as physical elements at orgasm and none have been found to be useful markers of orgasm.
As I often say, ignoring or not capturing pelvic muscular data creates a situation in which researchers could end up blindly combining data about two physically different instances of 'orgasm' - one that includes rhythmic pelvic muscular activity and one does not. Conclusions made from this combined data without specific understanding that it is, in fact, combined data, is problematic. To me it's like making conclusions about what types of people have heart attacks using data from self reports not confirmed by doctors. What if there were people who actually had panic attacks and not heart attacks in there. They may have all called them heart attacks, but physically they were different, and that would affect the results. I imagine that the results about how spinal cord injury affects ability to orgasm is similarly affected by this self-reporting method, and I think that needs to be kept in mind.
INTRO
- Up to this point there hadn't been a lot of studies about sexual functioning in females with Spinal Cord Injury (SCI), and there's been a lot of controversy about (1) if women with SCI can have orgasms and (2) the effect of the type and site of the injury
- For a long time it was believed women with SCI couldn't orgasm (it references a quote from 1978 saying that was mentioned)
- Since then, several studies have indicated that some women with SCI can orgasm, but they were all non-lab studies using self report
- One study recorded pelvic muscular activity (through anal and vaginal contractions) in women with SCI attempting orgasm. Of the 10 participants, 6 claimed orgasm and 4 of these women showed pelvic muscular activity. However, the details of the types of SCI were not clear, so it is not as useful and it could be.
- The team that did this study also did a study a couple years earlier where one woman with tetraplegia claimed orgasm from chest and breast stimulation. "An extreme elevation in blood pressure along with a slight drop in heart rate and minimal change in respiratory rate was noted." They didn't mention pelvic muscle activity.
- "Based on the lack of understanding of the characteristics of orgasm after different types of SCI and the accompanying physiological events, the present study was designed to provide a laboratory-based controlled evaluations of orgasm in women with SCI."
METHODS
Subjects
- 25 women with Spinal cord Injury (SCI), 9 able-bodied control women
- recruited from SCI magazines, local newsletter, etc.
- normal menstrual cycles, no gynecological or neurological surgery, free from psychiatric disorder, and medically stable
- mean age for able bodied subjects: 32; Mean years of education: 15.6
- mean age for SCI subjects: 34; Mean years of education: 15.1
- "all subjects underwent anal sphincter electrography and somatosensory evoked potential testing by a single examiner using Dantec Counterpoint equipment." (After I looked into this a bit, I think this means they were tested to check for how much control they each had over their anal sphincter muscles - whether they could contract it, etc.)
- all underwent comprehensive examinations by the principle investigator according to the International Standards for Classification of Spinal Cord Injury to assess their specific level of neurological impairment.
- A questionnaire developed by the investigators was given to participants to specifically assess the impact of SCI on sexual functioning.
- The Derogatis Sexual Function Inventory (DSFI) was given to each participant to assess the quality of their current sexual functioning.
Equipment
- Participants were in a private wheel-chair accessible lab resting on a hospital bed in a hospital gown
- The following devices were placed on the participants for attaining measurements
- physiologic electrodes
- A photoelectric pulse sensor on right big toe (to measure heart rate)
- thermocouple transducer (nasal respiration)
- automatic cuff (blood pressure)
- Perry Systems Perrymeter (rectal muscle contractions)
Study Protocol
- "Subjects underwent a 75-minute study protocol designed to obtain information on the physiological events accompanying orgasm."
- "Subjects were shown a sexually explicit video and were instructed to stimulate themselves to orgasm through any means possible."
- 2 subjects were unable to stimulate themselves, so were stimulated by a partner
- "Subjects were asked to verbally indicate when they experienced orgasm and when they desired to stop stimulation, either with or without achieving orgasm. If subjects were unable to achieve orgasm withing 75 minutes, the session was terminated."
ANALYSIS
- "Appropriate descriptive statistics were used to characterize study participants in each of the study groups. Differences were examined both within and between subject groups."
- Then there are some details about which statistical methods were used
RESULTS
- Participantswere categorized in 4 groups
- Group 1 - complete SCU
- Group 2 - incomplete subjects with preserved light touch sensation in the T11-L2 dermatomes
- Group 3 - incomplete subjects with preserved pin prick sensation in the T11-L2 dermatomes
- Group 4- Able-bodies controls
- Dependent measures include
- Heart Rate (HR)
- Respiration Rate (RR)
- Systolic Blood Pressure (SBP)
- Diastolic Blood Pressure (DBP)
- No significant difference between any of the groups for HR, SBP and DPB at baseline
- There was also no difference between any of the groups for any of the dependent variables at time of orgasm.
- HR and RR was greater and DBP stayed steady at orgasm vs. baseline measurements for both able-bodied and SCI participants
- SPB stayed steady for able-bodies and was greater for SCI participants
- However, breaking the HR, RR, DBP, and SBD measurements down at orgasm vs. baseline within the different SCI groups, gives more varied results. (see table 2 below)
 |
| Sipski et al 1995 Table 2 |
- All 9 able-bodied participants had orgasms
- 4 of 11 had orgasms in Group 1 (complete SCI)
- 4 of 6 had orgasms in Group 2
- 5 of 8 had orgasms in Group 3
- "...whether the subject had an orgasm seemed to be related to whether there was a SCI, but not to the degree or type of SCI."
- For subjects that reached orgasm, there was a significant difference in time to reach orgasm between: SCI subjects w/ no lower extremity function, SCI subjects with some lower extremity function, and those without SCI.
- "An additional Chi-Square analysis was conducted to determine if the ability to have voluntary rectal contractions was related to rectal contractions at time of orgasm. Results were not significant." (me: meaning there were people who either did not have rectal contractions at time of orgasm but could voluntarily contract their anal sphincter and/or there were people who could not voluntarily contract their sphincter but did have anal sphincter contractions at time of orgasm - and there were enough of these people to show those two things didn't correlate strongly with each other. However, there was no raw data or further detail about this.)
- Subjects were asked to describe how they stimulated themselves to orgasm, where and how they felt their orgasm and what feelings were associated with the orgasm. (See table 4)
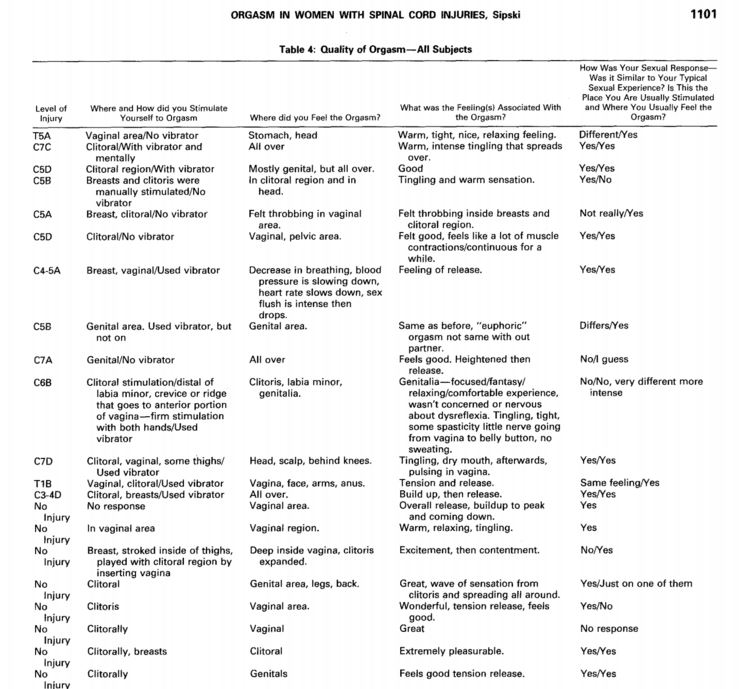 |
| Sipski et al 1995 Table 4 |
- All the subjects, regardless of whether their SCI was complete, chose some type of genital stimulation with the majority of subjects choosing clitoral stimulation.
- There was no consistent pattern for where the subjects felt the orgasm, and descriptors of the orgasm were generally similar between SCI and able-bodied women.
- "All but 2 women indicated this was a typical sexual experience for them."
- The DSFI that the participants took is a multidimensional test designed to measure the current level of sexual functioning, pcomposed of 10 subtests; measuring thing like "Sexual Information" (patient's general knowledge of sexual functioning), "Sexual Satisfaction" (the degree to which patients are gratified by their sex life), "Sexual Role" (balance between subjects masculine and feminine characteristics), and "Sex Drive" (patient's interest in sex as determined by frequency of various sexual activities).
- SCI patients scored significantly higher on "Sexual Role" but significantly lower on "Sexual Satisfaction" than able-body patients.
- Subjects who orgasmed scored higher on "Sexual Information" and "Sex Drive."
 |
| Sipski et al 1995 Table 5 |
DISCUSSION
- 52% of women with SCI were able to stimulate to orgasm, and women were able to orgasm no matter the pattern or degree of SCI. Both are consistent with the authors' previous work.
- "This information should help to dispel the myth that women with SCI, especially those with complete injuries, cannot achieve orgasm. We must, however, remain cognizant of the fact that a significantly lower percentage of women with SCI were able to achieve orgasms in the laboratory than our able-bodied control subjects."
- "No consistent characteristics were identified that would allow prediction of which women with SCI would to experience orgasm...thus both women with complete and incomplete injuries should be considered candidates for sex therapy aimed at improving their ability to achieve orgasm."
- It then notes that because women in the study who had better sexual knowledge were more likely to orgasm, that sexual education is important.
- "The majority of women in this study stimulated themselves in the clitoral and vaginal regions, similar to those women who were able-bodied. Although we often hear that breast stimulation is preferred by women with SCI, only 4 women with SCI in this study reported using breast stimulation in conjunctions with genital stimulation to achieve orgasm. Thus, as clinicians we may use this information to educate our patients with SCI about what methods other women find useful."
- The study notes that traditional sex therapy teaches women to achieve orgasm through body exploration and masturbation, but it is uncommon for clinicians to recommend masturbation to their patients with SCI. Yet all but 2 (because they needed partners to stimulate them) of the 13 orgasmic women with SCI achieved orgasms achieved it through masturbation and 8 of the 13 used a vibrator.
- "Based on these results, we recommend that women with SCI should be counseled as to the acceptability of masturbation and use of a vibrator. Providing them with a vibrator may also eliminate the 'embarrassment factor' associated with the purchasing a vibrator and would allow women to decide on their own when and how they choose to use it."
- "Women with SCI took longer than able-bodied women to reach orgasm. Furthermore, women with no voluntary movement in their legs required the most time, followed by women with some movement in their legs. An important implication of these results is that patients should be counseled to stimulate themselves longer if they are going to achieve orgasm."
 |
| Sipski et al 1995 Table 3 |
- Women with SCI showed similar HR and RR responses to able-bodies women, but showed higher blood pressure during orgasm. "The reason for the greater blood pressure responses may be related to the level of injury of our subjects, because all these women are prone to autonomic dysreflexia with intense stimulation below the level of injury. These responses, though greater than those of able-bodied women, were in no case dangerously high, and should serve as documentation that it is relatively safe for women with SCI to use a vibrator for self-stimulation."
- The final issue the paper discusses is what this all means about which neurological and physical things negotiate orgasm. "Obviously if women with complete SCI can stimulate themselves to orgasm through upper body stimulation, the neurological stimulus must originate in the brain or above the level of injury. In contrast, if SCI women can stimulate themselves to orgasm through genital stimulation, then reflex autonomic activity is likely to be involved. This report supports the later conclusion..."
- And the final paragraph concludes: "The findings of our study are encouraging in several respects. Women with SCI are able to be stimulated to orgasm in the laboratory under conditions of self- or partner-stimulation. Their ability to achieve orgasm is not related to the degree of injury; furthermore the physiological correlates of orgasm are not dissimilar to those of able-bodies women. We are unable to specify predictors of orgasmic ability in post-SCI women, but with the information available, it is worthwhile to attempt treatment protocols. Along with the development of these protocols we should continue to examine the neurophysiology of orgasm after SCI, and to use this information to help individuals with their disabilities."
MY THOUGHTS
This is clearly useful and impactful research about sexual function in women with SCI. It dispels previous notions and shows details about how women with SCI actually do stimulate themselves.
It is also interesting as a piece to understanding the neurological and physical things that are involved with orgasm. However, I think that aspect of this article is weakened by the choice to not include details about pelvic muscle activity at orgasm. As I often point out in this blog, due in no small part to the confusing way in which female orgasm is taught and discussed, a woman merely saying that she orgasms does not necessarily mean that she physically has orgasmed. So, when 2 women claim orgasm, one may be describing an event that includes the rhythmic pelvic muscular activity that is understood as the physical aspect of orgasm, and the other may be describing a pleasurable feeling that does not include those rhythmic pelvic muscular activity.
It is not a problem for researchers to acknowledge that both can be valid, pleasurable experiences. However, it is absolutely a problem to blindly lump data from these two physically different events together and make scientific conclusions about the physical qualities of orgasm. It is just plain bad experimental design and any physical conclusions based on that type of experimental design is mushy and messy at best. I mean, it is just true that an 'orgasm' that involves the rhythmic pelvic muscular activity is different than those that do not, and thus could very likely have different catalysts, mechanisms and involve different neural pathways. Maybe all the claimed orgasms in this study where similar enough in the pelvic muscular activity department to lump together, but maybe they weren't, and the authors (as is the case with so many authors of female orgasm studies) do not feel it important enough to mention one way or the other.
Now, I would assume, and this is only my assumption, that since these researchers collected this pelvic muscle data but did not report it, that they probably found that some of the women did not display rhythmic pelvic muscular activity at the time of orgasm. I would further assume that they chose not to deal with this inconvenience because pointing out that some women didn't have these pelvic contractions even when they claimed 'orgasms' would seem like they were judging and invalidating the experience of 'orgasm' had by those women. I get it. I do, and I also think that is a common reason why this aspect of female orgasm is so often ignored - niceness and terror of being accused of not believing women's descriptions of their own experience (at least I hope it's that and not simply for convenience of conclusions). However, it's lame, and it's got to stop. This is scientific investigation, and physical knowledge of female orgasm will continue to linger in mushy, wishy-washy confusion if the science continues to be half-assed in this way. If some of these SCI or able-bodies women didn't display pelvic muscular activity, then the physical qualities of orgasm between the two groups necessarily should be investigated and concluded about differently.
So, that's my two cents. It seems to always be my two cents about orgasm studies, but seriously, I mean seriously, the scientific value of being clear about the physical qualities of the phenomenon one is studying before one makes physical conclusions about it, is pretty much so obvious that it makes me feel super suspicious about why it's not obvious to the researchers and reviewers involved with these studies. For real though, it's an obvious problem that no-one seems to care about or even notice.
No comments:
Post a Comment