Here is another installment of A Journal Article I read. This one is about an article I've been meaning to do for a long time. It's one that's used A LOT in articles (everything from crappy web articles to the background parts of other journal articles), TV segments, and in even debates with me as proof that there is stuff up in the vagina that can actually make women orgasm. Also, this is an article with Beverly Whipple and Barry Komisaruk as authors. Both are very active in the media and often pop up as the the expert in articles about female orgasm. Whipple was one of the 3 authors of the G-Spot and Other Recent Discoveries About Female Sexuality - the book that introduced the G-spot and female ejaculation to pop culture. Komisaruk is a scientist in the psychology department at Rudgers and has been researching about females and orgasm for a long while - working closely with Whipple actually since at least the early 90's. This seems to me to be their most famous work.
Brain activation during vaginocervical self-stimulation and orgasm in women with complete spinal cord injury: fMRI evidence of mediation by the vagus nerves.
Komisaruk BR1, Whipple B, Crawford A, Liu WC, Kalnin A, Mosier K. Brain Res.
2004 Oct 22;1024(1-2):77-88.
The Quick Version
I'm going to give a quick overview for those of you who don't like the details. I actually think this research into women with Spinal Cord Injury (SCI) is pretty cool stuff - and probably promising for many women with SCI (There's also another good study about women with SCI and orgasm HERE. I'll review it eventually, but check it out if you're interested)
In this study, 5 women with Spinal Cord Injury (SCI) were given cervical stimulation. And...it’s a particular kind of cervical stimulation that involves a pessary, which is kinda like a hard cervical ring that had to be professionally fitted to each woman individually. The pessary has Velcro on it, and a device that ends with a modified tampon with Velcro on the end is inserted in and attached to the Velcro on the pessary. It is controlled by the patient and sort of puts suction-y pressure on the cervix (without really touching the cervix - cause that hurts like a bitch, right?). It’s not your average vaginal stimulation, ya know? Three of the five women verbally reported orgasm which was accompanied by an increase in brain activity in places the researchers felt, given some past studies, were consistent with what would be expected during orgasm. Heart rate, respiration, and blood pressure were not measured and neither was pelvic muscular activity. They suggest the Vagus nerve bypasses the spine and makes this possible even with the spinal injuries.
So, the study supports a very particular type of cervical stimulation having some amount of direct pathway to the brain. However, 3 of the 5 women claimed that this cervical stimulation caused an orgasm also. Increased brain activity was found at the time these 3 women claimed to orgasm, and that was seen as proof that the orgasm happened. However, as of yet there is no clear understanding of whether that brain activity is a reliable marker to indicate any particular kind of climactic sexual experience, much less the muscle contractions identified by M&J’s work (which were not tested for directly either). There is also no understanding of what that brain activity correlates to physically, or if it correlates to anything physical at all. Although a kind of cool study, it does not show proof for vaginal or cervical stimulated orgasms as is often suggested.
The Details
Background
The background discussion mostly focuses of whether or not there is direct connection between the brain and female genitals. It points out evidence in rat studies that basically say there seems to be a direct connection through the Vagus nerve between the cervix / uterus and the brain - meaning that it doesn't first go through the spine. They say this because there were some stimuli that could still be detected in these rat's brains even when the spine was severed in a place that should not allow stimulus detection that far down their bodies. It goes on to say that until this article there was no evidence that this was true in humans also.
The Experiment
The 5 women ranged in age from 23 to 54 and there time with SCI ranged from 1 to 21 years. They were all found to be healthy both physically and mentally. They were also examined to ascertain the level and completeness of the SCI using standard methods.
"Individuals were imaged in the coronal and sagittal planes using standard functional MR imaging BOLD techniques....Individuals' heads were immobilized with foam and taped to the head holder to limit motion."Each woman first went through a series of tests in the MRI as a sort of control to demarcate the Nucleus Tractus Solitarii (NTS) region of the medulla oblongata. This was done because that is where the Vagus nerve is known to project, and the hypothesis is that the cervical stimulation will project there too since it is believed that the Vagus nerve is carrying the stimuli directly to the brain. This was done by having the women perform activities that are known to project on or near the NTS. These included things like tapping a finger and tasting sweet, sour, salty and bitter.
The women later self stimulated their cervix, using the contraption described above (I also added a quote with the specifics of this device at the end of this article), and MRI images were taken during the process. There is no information given about how long the women were allowed to stimulate their cervix or if there were particular instructions for the process.
Results
Basically, theses authors found that there was, as expected, activation in the projection zone of the Vagus nerves during the time the women were applying Cervical Self Stimulation (CSS). It was found to be in the lower part of the NTS which means it was lateral to the area activated by taste sensations (which is expected to be in the anterior part of the NTS) and it was adjacent to the part activated during finger tapping (which was expected to be in the nucleus cuneatus which is next to the NTS).
 |
| Komisaruk et al. Brain Res. 2004 Oct 22;1024(1-2):77-88. |
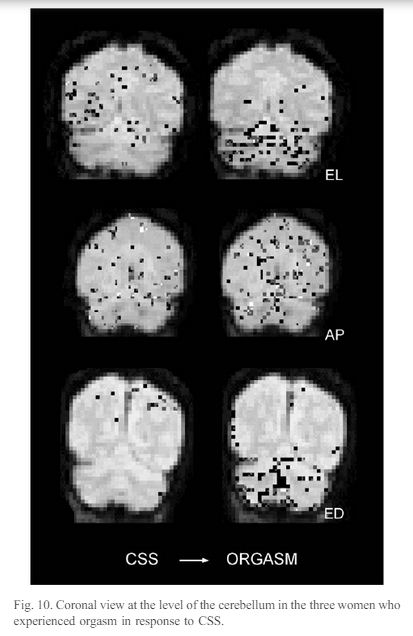
For the 3 women who claimed to orgasm, there was gradual increase in brain activity, from onset of CSS to orgasm. It doesn't really give data about if there was or was not an increase in brain activity during CSS for the 2 women who did not orgasm, and it did not compare the brain activity of the women who did and did not orgasm. There was also no discussion of how long each of these women engaged in CSS - except that EL went from CSS onset to orgasm in about 8 minutes.
 |
| Komisaruk et al. Brain Res. 2004 Oct 22;1024(1-2):77-88. |
All of the women reported a sensation when the stimulator was placed against the pessary on the cervix, although they each described it a little differently. AN described a feeling of changing pressure, VA described a "chill inside," AP and EL described a "touch inside," with EL also feeling vaginal muscle contraction at that time.
The women were also checked for pain threshold during the cervical stimulation compared with resting pain threshold. I know from reading their prior studies focused exclusively on this test that this was ascertained using a device to put increasing pressure on the fingertip, but strangely I couldn't find anything about the experimental method for this in the study even though the results were reported here. The authors tell us each woman had increased pain threshold during the cervical self stimulation. It seems weird to me that it's not in there, but I'm not too worried about it since I've seen one of their studies on it before - which I will review soon.
Discussion
The discussion first focuses on the spinal injuries each women has and whether it seems clear that the brain activation that occurred during cervical self-stimulation could be confidently said to have occurred through direct brain-cervix access by the Vagus nerve. The later part of the discussion mostly focused on what other studies showed about brain activation during orgasm and arousal.
"There appeared to be an overall increase in brain activation at orgasm in the present study in which activation of specific and multiple brain regions could be discerned...Differences between regional activation during, versus before or after, orgasm suggest that areas more directly related to orgasm include paraventricular area of the hypothalamus, medial amygdala, anterior cingulate region of the limbic cortex, and region of the nucleus accumbens. At present, we cannot distinguish whether these regions are activated uniquely at orgasm, or whether their activity increases gradually, only exceeding an arbitrary detection threshold at orgasm."
 |
| Komisaruk et al. Brain Res. 2004 Oct 22;1024(1-2):77-88. |
The authors go on to tell us there is no known evidence of orgasm in rats, but compares the brain scans in this study to those of cervix stimulation in rats.
Below is the only discussion about how previous studies about brain imaging during orgasm match up to this study.
"To our knowledge, this is the first evidence of activation of hypothalamus during orgasm in men or women. Earlier reports of orgasm in men found activation in prefrontal cortex, but not subcortical structures [74]. Recently, Holstege et al. using positron emission tomography reported that during orgasm, elicited in men by penile stimulation by a partner [21,24] and elicited in women by clitoral stimulation by a partner [25], the mesodiencephalic region, cerebellum, and several cortical areas, but not the hypothalamus, became activated."The authors then discuss a prior study by Wallet et al. of men during sexual arousal - not orgasm- caused by visual stimulation. The fMRI in this study, "reported that activity was increased in the amygdala, hippocampus, hypothalamus in men relative to women, wheras the striatal regions (candate and nucleus accumbens) were activated in women."
I am no brain fMRI expert or neuroscience expert here, but from the past data they are comparing this to, it seems like the activation they are seeing might be as close to the studies capturing visually stimulated arousal as it is to the studies capturing orgasm. I might be wrong here, but it just didn't seem like the activation observed in this study were clearly types of activation that indicates orgasm .
The the authors go on to discuss brain areas activated in this study that may indicate oxytocin release. However, as they themselves mention, oxytocin release, although part of orgasm, is also part of all kinds of other things, including vaginal or cervical stimulation (known as the Ferguson Reflex). They then make connections with the oxytocin release and the women's increased pain tolerance, and talk more about what might be involved in that increased pain tolerance observed in this study. The only other part of the discussion that involves itself with orgasm specifically is the following assertion.
"A salient and reliable feature of brain regions activated during orgasm was activation of the cerebellum. The cerebellum modulates muscle tension via the gamma efferent system, and it receives proprioceptive information [45]. Since muscle tension can reach peak levels during orgasm [44] and contribute to the sensory pleasure during orgasm [31,32], it is not unlikely that the cerebellum thereby plays a significant motoric and hedonic role in orgasm."
So, it seems the authors are pointing to the activation in the cerebellum as the most important and reliable indication that an orgasm really did happen. They point to this because the cerebellum deals with muscles. It's funny to me because when they say this, they cite Masters and Johnson's Human Sexual Response (that's the [44]), which means to me that they are acknowledging that the rhythmic muscle activity that Masters and Johnson identified as a reliable marker of orgasm, is in fact quite important and reliable. It's funny to me because these authors have a long track record of advocating for widening the scope of what the word 'orgasm' (particularly female orgasm) means beyond the very clear, observable, and widely accepted definition Masters and Johnson set out in the book cited above. They also have a long history of not checking for or even really discussing that reliably observable marker for orgasm in their studies about female orgasm.
So, maybe the brain activation in the cerebellum during the reported orgasms in this study is an indication of the muscular activity of an actual, Masters and Johnson defined orgasm, but maybe it's not. We don't really know much about what exactly the brain activation indicates or whether we could count on any parts of that brain activation to accurately and reliably mark orgasm. However, if these authors really wanted to prove that these women had orgasms and that the activation seen in their brains were truly related to orgasm, then they could have just checked. It is absolutely possible to do so, but they did not.
Conclusion
And that brings me to the conclusion. I'm on board with their statements like, "In women, the Vagus nerves provide a genital (vaginal-cervical) sensory pathway that bypasses the spinal cord." I think that's fair given the data they collected in this study.
I'm not cool, however, with their conclusion that, "in cases of compromise of vagina-cervical sensory activity via the genitospinal nerves, genital sensory activity conveyed via the Vagus nerves is evidently adequate to induce orgasm in women."
I think that indicating a particular physical stimulation causes orgasm when an orgasm has not been verified is a bit irresponsible (even though tons of researchers still do it). These authors' findings of extra brain activity when a woman says she has orgasmsed is not enough to make that conclusion. This is a scientific investigation, and the bottom line is that asking a person whether or not a particular physical event happened in their body is simply not good enough. It's a start - not a conclusion.
The data they collected is certainly worthwhile, and could be important for further research, but claiming that these women stimulated their cervix to orgasm is at best contentious. There is no evidence that what these women experienced involved the rhythmic muscle activity known to be a reliable, accurate marker for an orgasm. There is not even evidence that the brain activation identified in this study is a reliable or accurate marker of anything at all - much less orgasm.
This study, to my dismay, does as most studies about inner-vaginal stimulated orgasms do. It does not actually confirm an orgasm takes place. It's easily detectable, but too often in studies about female orgasm, the researchers simply don't bother. There is a physical thing called an orgasm, and we acknowledge that this physical thing is an orgasm when we talk about males. However, for females it seems like any time a woman says she orgasms, then we must include whatever it is that she experienced at that time within the definition of the word orgasm. It's really, like, the worst way to go about scientific inquiry, like just the worst. One person could literally be using that word to describe something completely physically different than another person. Yet, scientists are investigating, speaking about, advising on, and making conclusion about all those different 'orgasms' as if they are the same things. I mean, how could there be any confusion or miscalculations involved in that?
This lack of verification might just seem like a small experimental choice, but it is much more. If the women in this study say they orgasm, but they are actually not exhibiting rhythmic muscle spasms, then those women are experiencing something different than women who do experience the rhythmic muscle spasms - and their experiences should not be called the same thing or discussed in the same way. Some things are the same, and some things are different. The scientific community should acknowledge when things are the same and different. It's not a hard concept. Debate about the value of these two different experiences or what to call them is absolutely valid, but if the scientists doing research in this area are intentionally refusing (as I worry some are) to even gather information about what I know they know is important to a clear understanding of how female sexual release works, then I call bullshit. This area of study, and women, deserve better.
Appendix (in case you want to know more about that cervix stimulator)
"Vaginal-cervical self stimulator was applied with a passive stimulator consisting of a handle into which a modified tampon mounted on a lucite rod was inserted at right angles. A Velcro disc was attached at the tip of the tampon. To a ring pessary (Model PRSFS, Milex Products, Chicago, IL) previously fitted to each subject by her gynecologist, was attached by suture silk a matching Velcro disc. The pessary was inserted by a registered nurse and the Velcro disc attached to the tampon stimulator was pressed against the matching Velcro disc on the pessary. This device centered the stimulator tip against the cervix through the pessary and the pessary protected the cervix."
Thank you for another brilliant debunk of a widely quoted and cynically misleading “vaginal orgasm” story.
ReplyDeleteThat they sewed a piece of Velcro to the cervix confirms medical knowledge that the cervix is a sensory dead zone, not a site of orgasmic nerves. Women who claim to have cervical orgasms either don’t know what an orgasm is, or are actually getting clitoral stimulation from grinding their clitoral area against the male pubic bone area, or simply lying to themselves or the researchers to appear “normal” or very sexy.
What do you think has engendered a whole cottage industry of vaginal orgasm seekers? And why do women participate in this, contrary to their own experience and knowledge of female anatomy?
Keep up your great work on this blog. I think that you and Vincenzo Puppo are the only sex authorities who have not fallen into the “there’s gotta be an orgasm in there SOMEWHERE!” crowd. It’s a reign of error that started in about 1980, with a group of neo-Freudians inventing the “g-spot,”, and is now fueled by the “crura legs” folks and the CUMD believers.
Thank you again for taking these “research” reports apart with your smart, careful analysis.