Welcome back to An Article I Read. In this series I read a peer reviewed journal article that relates to female orgasm, and then I write a summary of it for you. I do my best to be thorough, but I also try to make it shorter and more comprehensible than reading the actual article. I do way too much googling and re-reading in my attempt at achieving that, but still this is by far my favorite series in this blog. I wish I had more time for these. I will also give you my opinion about the article, but when I do, it will be clearly marked under a heading ('My opinion' for instance might be one such heading) or I will put them into these brackets [me: ] so that you know it's my opinion and not something in the article. Otherwise, everything I write will be as best a summary of something said in the article as I can do, and all things quoted are from the article.
What is the "true" prevalence of female sexual dysfunctions and does the way we assess these conditions have an impact?
Hayes RD, Dennerstein L, Bennett CM, Fairley C. J Sex Med. 2008 Apr;5(4):777-787.
My opinions about why this is being studied
Female Sexual Dysfunction (FSD) has a history of being a bit of a contentious thing - from hysteria to Freud's clitoral vs. vaginal orgasm ridiculousness to modern concerns about if drugs can help with FSD. The particular contentiousness I want to point out in relation to this article, though, is one that's gained a lot of traction in recent years. I'll summarize it as I understand it:
Are we defining Female Sexual Function based on our understanding of male (and not female) sexual functioning? Particularly, are we assuming that the sexual response cycle of desire - arousal - orgasm - recovery that's been used for years is as accurate for females as it is for males when it may not be?
some background
Now this article I'm summarizing is really about seeing if the way we measure the percentage of women suffering from FSD will change depending on the method that is used. However, I think the interest in researching this (outside of simply being a fabulous and I would say necessary type of scientific investigation into anything one is studying) is that there has been a slow push in the field to consider that maybe women are just naturally not going to "automatically" have desire pop up that induces physical arousal the way men are. There is a growingly popular idea out there - that some people's (but mostly women's) sexual cycle tends to be different, where desire more arises from physical arousal than the other way around. There's a whole book on this that people love, but the gist I'm getting at here is that if women aren't really going around with a bunch of sexual desire and arousal the way men are, then maybe that's not dysfunction - maybe that's normal.
So in this article I'm summarizing here, one of the ways that the researchers use to determine FSD is with a questionnaire that only classifies a woman as having FSD if she has low sexual function and sexual distress. So whereas traditionally questionnaires (and all the methods tested here to look for FSD in these women are types of questionnaires) tended to look merely at low sexual functioning (i.e. not feeling sexual desire, not being able to get wet, not being able to orgasm, sexual pain during sex), they included one that found out if a woman also had distress about the lack of desire, wetness or orgasm or pain during sex. If she wasn't distressed about it, she wasn't classified as having Female Sexual Dysfunction (SFD). When that extra criteria is added, and the American Psychiatric Association does now say that criteria should be added, the % of women identified as having FSD is much less.
It's a little subtle, but important. If women aren't distressed by their sexual functioning, why would we call it a dysfunction at all? Why doesn't it make more sense to adjust our understanding of FSD than to force women into dysfunction who don't feel dysfunctional (think how psychiatrists used to think about gay people. It was a dysfunction because they said it was - not because it necessarily felt dysfunctional to the gay person).
I'm just giving you some background and context as I understand it because I think it's interesting. I actually like the thinking out of the box here that this type of consideration brings. I think we should continue to deeply consider in what possible ways women's sexuality and sexual function is being measured and researched and judged based more on our understanding of male experience as opposed to the reality of female sexual functioning.
but....
That said, I also want to throw in that I worry a little about settling with the idea that a lot of women's desire tends to be 'different' from a lot of men's in that it doesn't happen quite so often or spontaneously and that desire often follows physical arousal rather than preceding it. I applaud backing away from tagging women that don't meet our traditional understanding of how and when desire arises as dysfunctional if they don't feel dysfunctional. However, I do think it's worth considering more deeply why there might be this tendency in women.
I think stepping back a bit and saying, 'why might women's desire tend to follow this pattern and men's tend not to?' is important. If we don't step back and consider that, I think it'd be easy to assume it's just a innate biological difference, and I imagine that is what a lot of people believe at least to some degree. I also imagine there is comfort in believing it is an innate difference because it seems non-problematic if it's 'just our nature.' However, there's lots of reason to assume that how women experience our sexual culture deeply affects how we express and understand our desire, arousal, and orgasm.
I mean, it's a cold hard fact that women don't orgasm during sexual interactions nearly as much as men - and not because women's bodies are less capable of orgasm than men (They are not. Women can orgasm as quickly and reliably as men during masturbation). So, that really simple reality alone gives me pause about attributing female desire patterns to our innate qualities. I mean, clearly many past experiences of sexual encounter + orgasm (a lot of male experiences) are WAY better at training you to be aroused when considering the possibility of a future sexual encounter than sexual encounter + NO orgasm (a lot of female experiences). Also just consider for hetero folks how much more common it is to see a woman sexualized vs. a man. Life itself is just kinda less sexy for hetero women in general. My point is, I don't want this very important inquiry into how we define sexual dysfunction in women to also act as a way to cover and sanitize a very nasty reality; that female orgasms are at a disadvantage in our culture and the effects of that ripple out and negatively affect all aspects of sexual culture - including women's ability to feel desire.
In short, lots of women have particular patterns of desire and arousal different from men and it doesn't mean we are lesser or wrong, but it very well might mean that we were forced to develop our desire in the way we do because we existed in a shitty sexual culture that ignored our clit for our vag-hole. We ladies are making lemonade out of lemons, but maybe we can use this knowledge to just give the next generation of ladies pre-made lemonade instead of giving them lemons and telling them it's just as good as getting the lemonade already made.
So that was a lot of background. I think it's interesting though, so I wanted to touch on it before I summarized the article. BTW - enjoy the summary below.
Introduction
- The true prevalence of Female Sexual Dysfunction (FSD) is contentious. Studies have tracked it at anywhere from 8% to 55%. Although these differences could be due to the different populations studied, it also very well may have to do with differences in how FSD is studied.
- For instance, when researchers ask for only longer lasting difficulties in studies, FSD rates tend to be lower
- Also "the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorder fourth edition stipulates that both low sexual function and sexual distress need to be present in order for a diagnosis of FSD." However validated measures of sexual distress were only created recently and a lot of previous studies don't include it, so there is a problem with lack of standardization in FSD rates.
- Previous research indicates incorporating sexual distress measures in these FSD surveys shows a lower prevalence of FSD.
Aims
To compare in detail the results of 4 different surveys on the same group of Australian women in order to determine if the differences in the surveys help explain the differences in FSD rates. The surveys used will help determine the impact of multi-item instruments (meaning questionnaires), simple questions, different recall periods, and the inclusion of a sexual distress component.
Method
- The questionnaire used for this study was the 2005-2006 Australian Study for Understanding Women's Sexuality and Health (ASUWSH).
- Self-administered questionnaire to collect information on sexual function and sexual distress along with demographic and risk factor data
- 1002 randomly selected women ages 20-70 with basic English literacy, and registered to vote (in Australia 98% of people are registered) received a package with a cover letter, participant info sheet, the questionnaire, brochure about related medical services, and a return slip.
- Participant details were included on return slip but not questionnaire, and they were returned separately so that the questionnaires remained anonymous but researchers could identify who completed a questionnaire
- Participants had option of receiving a cinema ticket and/or a report of the study's final findings
- Those that didn't wish to participate indicated on the return slip and were not contacted further
- If they didn't receive a return slip within a month a 2nd package was sent. For 100 women who hadn't responded to 2 packages a 3rd was sent, but the return rate was so low, they didn't send a third to any others that were not heard from
- Packages sent to 102 randomly selected women also included a delivery confirmation to see how many packages did not make it to the destination.
Main Outcome Measures
The survey included a variety of sub-questionnaires with question styles that are typical of questionnaires in previous FSD studies. These are the styles included in the Survey (followed by the reasoning for including it in parenthesis)
1. Questions asking participants to report sexual difficulties that happened within the previous month (to represent simple questions where respondents are asked to report 'problems' or 'difficulties' within a recent period of time)
2. Questions asking participants to report sexual difficulties that happened for at least a month within the previous year (to represent simple questions where respondents are asked to report 'problems' or 'difficulties' but within a longer time frame)
*both 1 and 2 asked if participants had experienced any of the following for each of the time frames
lacked interest in having sex
had trouble with vaginal dryness
were unable to come to orgasm (a climax)
experienced physical pain during intercourse
3. Included an 18 question abbreviated version of the Sexual Function Questionnaire (SFQ), a "validated, self-report, multi-item scale that employs a cut-off scale to determine if women have experienced low sexual function in the previous month" (to represent a multi-item scale questionnaire used to measure sexual functioning that classifies those scoring low sexual functioning as having FSD)
4. Included the Female Sexual Distress Scale (FSDS) questionnaire, a "validated, multi-item scale that employs a cut-off score to classify women with sexual distress experienced within the previous month." (This combined with the SFQ, together they call it SFQ-FSDS, represents questionnaires that only classify women experiencing both low sexual functioning and sexual distress as having FSD.)
The SFQ was first in the survey, followed by the FSDS, and then the two versions of the simple questions. Demographic and risk factor questions were dispersed throughout.
Analysis
- The SFQ employed both arousal-sensation questions and arousal-lubrication questions, but the sets of simple questions only included vaginal dryness questions in relation to arousal disorder. So, the arousal-lubrication questions in the SFQ were used for comparison and the arousal-sensation questions were ignored.
- All women were asked to answer all sections of the questionnaire even if they had not had any sexual activity (sexual activity includes masturbation) during the period in question.
- Women with no sexual activity during the period could be classified as having a desire problem but could not be classified as having arousal, orgasm or sexual pain problems. The exception to that is women who had no sexual active because of sexual pain worries. These women (if they didn't have desire or pain problems) were kept in the study and classified as free of FSD instead of being classified as missing data points.
- prevalence estimates (the percentage of women displaying these FSD sub-catagories) and 95% confidence intervals produced by each questionnaire style for the following: hypoactive sexual disorder disorder (HSDD) aka low sexual desire, female sexual arousal disorder (FSAD) (using vaginal lubrication answers as indicators), female orgasmic disorder (FOD), and dyspareunia aka sexual pain problems.
- The SFQ-FSDS results (results that used both low sexual functioning and sexual distress to classify a woman with SFD) were compared to the other styles of questioning in all the above categories. The SFQ-FSDS was used as a 'gold-standard' to compare against because it has been well validated and also reflects the current recommendations for diagnosing SFD.
- If a question related to one of those categories was left empty on an otherwise completed questionnaire, it was simply not used, which lowered the answer rate for some categories, but never lower than 95% of the total number of questionnaires included in the study.
- The 2 types of simple questions, each employing a different recall time range, were also compared
- In addition, the previous month recall version of the simple question was compared with the SFQ (which also employed a month recall). Both of these did not include questions about sexual distress
Results
- The researchers were able to estimate the number of women that did not ever receive their packages (due to out-of-date address, lost mail, or recipient being deceased), by investigating the package fate for the 102 random women that were chosen to have Postal Service Delivery confirmation. From this, it was estimated that 756 women actually received their package
- Based on above estimate, 45% (356) of respondents completed and returned the questionnaire
- The table below (table 2) shows the results for prevalence estimates (%) among the respondents across the 4 types of questionnaires for each of the different sexual dysfunction types studies: hypoactive sexual disorder (HSDD) aka low sexual desire, female sexual arousal disorder (using vaginal lubrication answers as indicators), female orgasmic disorder (FOD), and dyspareunia aka sexual pain problems.
- It also shows the 95% Confidence Interval in the parenthesis next to the Prevalence %

- The SFQ-SFDS questionnaire showed lower prevalence % estimates than the other types of questionnaires for all 4 types of sexual dysfunctions.
- Comparing the 2 versions of the simple questions indicated that questions asking to recall if something occurred during the previous month showed lower prevalence % estimates in all 4 of the sexual dysfunction categories than if asked to recall if something occurred for 1 month or more from the previous year.
- Comparing the simple set of questions with a 1 month recall vs. the multi-item scale questionnaire (SFQ) which also had a 1 month recall, the multi-item scale showed higher prevalence % estimates for low sexual desire, low arousal (lubrication), and female orgasm disorder, but not for sexual pain.
- In total, 32% of women with low desire, 31% with low arousal (lubrication), 33% with orgasm difficulty, and 57% with sexual pain were also sexually distressed.
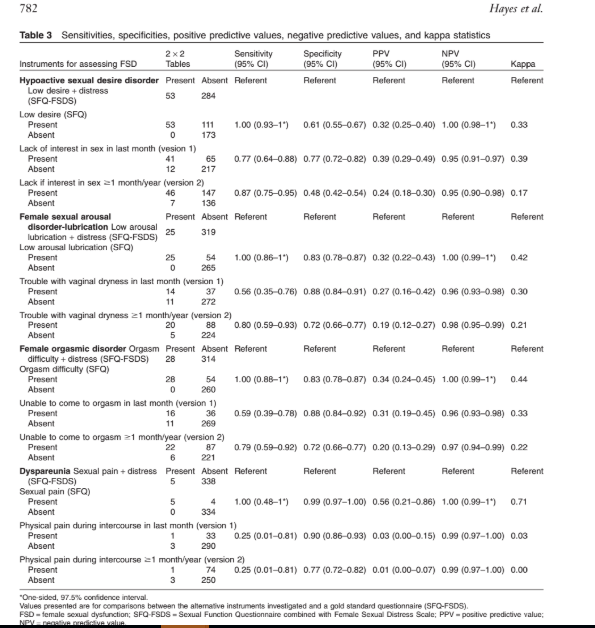
- [Me: the researchers also report kappa statistics, negative and positive predictive values, specificity and sensitivity statistics when employing the SFQ-FSDS as the gold standard questionnaire against the other types of questionnaires. I don’t feel knowledgeable enough about stats to speak much on them, but you can check it out in Table 3 below.]
Discussion
- "This is the first time that this range of instruments, frequently used for assessing FSD has been compared directly in the same study."
- Including "sexual distress" as a necessary element for diagnosing Female Sexual Dysfunction (FSD), as in the FSQ-FSDS questionnaire, reduced the prevalence estimates of FSD by 2/3 or more for all 4 categories. "In additions, these results indicated that only a portion of women with low sexual function (31% -57%) experienced sexual distress."
- "Changing the recall period from the previous month to one month or more in the previous year approximately doubled the prevalence estimates of all sexual disorders investigated."
- When comparing the FSQ-FSDS, the questionnaire that incorporated both low sexual function and sexual distress with the other questionnaires, the FSQ-FSDS "displayed a broad range of sensitivities and specificities across the different domains of FSD."
- "positive predictive values indicated that less than 60% of women classified as having FSD by alternative instruments [me: questionnaires] were experiencing FSD according to our gold-standard instrument (FSQ-FSDS)."
Limitations of the study
- The true gold standard of FSD is a clinical diagnosis, but with these anonymous surveys, that could not happen.
- The FSQ-FSDS was used as the gold-standard because it's well validated and reflects current definitions of Female Sexual Dysfunction (which includes having sexual distress). However, "the FSQ-FSDS is based on a current models of FSD," and "debate regarding which model best represents female sexual response and what constitutes FSD continues in scientific literature."
- The FSQ was validated on women age 19-65 but the abbreviated version (used here) was only validated on women age 19-49.
- The FSDS has not been validated on Australian women with FSD.
- "The America Foundation of Urological Diseases divides FSADs (Female Sexual Arousal Disorders) into genital, subjective, genital combined with subjective, and persistent sexual arousal subtypes. [me: see Puppo's take on the naming of persistent sexual arousal disorder] In our analysis, we only included the genital lubrication aspect of FSAD (as opposed to subjective arousal or the arousal sensation domain of the SFW). This was performed to allow us to make valid comparisons between instruments [me: questionnaires] as the simple questions we investigated (that were based on the questions from a frequently cited study by Laumann et al.) only asked about this particular aspect of sexual disorder. Not including subjective sexual arousal is a deficiency of both that earlier study and the present comparative analysis."
- "A further limitation is that the order of the instruments [me: questionnaires] used to measure FSD was not randomized. As all the instruments we investigated were included in one questionnaire, it is possible that participant's response to one instrument may have influenced their response to another. This may have artificially increased the correlation between instruments. Consequently, the true difference between these methods of assessing FSD may be even greater than our results indicate."
- Response rates for sensitive topics always tend to be low and seem to be decreasing over the years, but the overall response rate and prevalence estimates for FSD using the simple question section was comparable to previous studies of Australian women using the same simple question survey.
Strengths of this Study
- There was a variety of questionnaire types used that showed the impact of question type, recall period and inclusion of the sexual stress component on prevalence estimates
- The population was randomly sampled and the questionnaires employed have been extensively validated.
- Included all women in the sample, not just women who were currently sexually active
- These types of comparative studies for FSD diagnosis questionnaires are rare.
Learnings
- Previous studies show that prevalence estimates are lower when the time period for a sexual difficulty is raised (for instance asking about a particular sexual difficulty that lasted for at least a month vs asking about that same sexual difficulty but only if it lasted for at least 6 months). "Our data indicate that in addition to the duration of sexual difficulty the length of time over which women are asked to recall sexual difficulties also affect reported prevalence."
- That the inclusion of sexual distress in an FSD diagnosis has an impact on prevalence estimates is supported by previous research.
- The type of questions, the recall time employed, and the inclusion of things like sexual distress in the questionnaires that researches decide to use have important impacts on the results. "Consequently, reported associations between risk factors and FSD may also change depending upon the instruments researchers employ to measure FSD."
- "The absence of a standard, generally accepted, convention for determining the presence of FSD represents a major limitation in current research." However, there is still a lot of debate about what constitutes FSD and how to appropriately diagnose it, and researches would do well to keep this all in mind for future studies and as the definition of FSD evolves over time.
- "We envisage that this investigation will alert future authors to bias that may be introduced by the instruments they employ when conduction their own research. Also, we would like to make clinicians and researchers aware of the impact of instruments used to assess FSD when drawing conclusions based on published literature in this area."
Conclusion
Everything said in here was basically also said in the discussion.
[ME: As always, I'd like to point out something that should be way more obvious. Some (I'd venture to say most) Female Sexual Dysfunction (FSD) probably has to do with the fact that people don't truly realize that the clitoral glans area, and not the vaginal canal, is the female organ of sexual pleasure, just as the penis is for the male. And, because of that, way, way too many females are literally not getting sexual stimulation focused on the correct area of their bodies (like if males were mostly getting ball, not penis, stimulation) *and btw any penile or clitoral related organ on a body is the organ of sexual pleasure, so it's really no different for intersex folks that carry an organ more in between clit/penis.* Also, I'm just gonna throw this out there too - maybe some women don't describe themselves as distressed about their lack of orgasm, arousal, or desire because they live in a shit sexual culture that tells them and demonstrates to them all the time in all the different ways that women are less sexual, less capable of orgasm and harder to please - and maybe those ideas get internalized to a point where a woman might think that's just the way things are, so she settles into it...again, making lemonade out of lemons.]
Read this informative blog and seek Women Sexual Health Gainesville VA, if you experience extreme pain or are unable to have orgasm. PRP from your own blood is used in this therapy to address your problems. To schedule an appointment, call Lifestyle Physicians Warrenton right away.
ReplyDeleteRead this informative blog and seek Female Sexual Health Gainesville VA, if you experience extreme pain or are unable to have orgasm. PRP from your own blood is used in this therapy to address your problems. To schedule an appointment, call Lifestyle Physicians Warrenton right away.
ReplyDeleteNice blog, I recently had the lifestylephysicians O Shot Gainesville clinic and I am extremely happy with the results! The staff were very professional and made me feel comfortable throughout the entire process. The O Shot itself was quick and virtually painless, and I noticed a significant improvement in my sexual pleasure and sensitivity soon after the treatment. I appreciated that the clinic used only high-quality, FDA-approved products and followed strict safety protocols. Overall, I highly recommend the O shot Manassas to any woman looking to enhance their sexual experience and improve their quality of life, and the Gainesville clinic is definitely the place to go for this procedure!
ReplyDeleteBuy Ladygra 100 Mg is one of the best and trust medication to treat sexual dysfunction in females.
ReplyDelete